Lesion Characteristics
Lesion Size (diameter): 18mm
Lesion Location: Right Lower Lobe (RLL), GGO
Visible on Fluoro: No
Case Information
Full Procedure Time: 45 Minutes
Final Pathology Report: Acute Inflammation
Patient Background
A female former smoker presented with a lesion seen on two prior CTs six weeks apart. To determine the optimal treatment a diagnostic bronchoscopy was scheduled to obtain tissue samples from the lesion.
The Procedure
Planning
During the planning of the LungVision™ system, a preoperative CT scan is uploaded and the lesion is identified and outlined to provide the system with an estimate of its size, shape, and location before the procedure begins. Additionally, the LungVision system utilizes the airway information extracted from the preoperative CT scan to generate a virtual bronchoscopy (VB) that highlights the optimal pathway to the lesion for those seeking to use LungVision for navigation. In this specific case, the Ethicon MONARCH™ robotic bronchoscopy platform was employed to navigate to the targeted lesion.
Registration
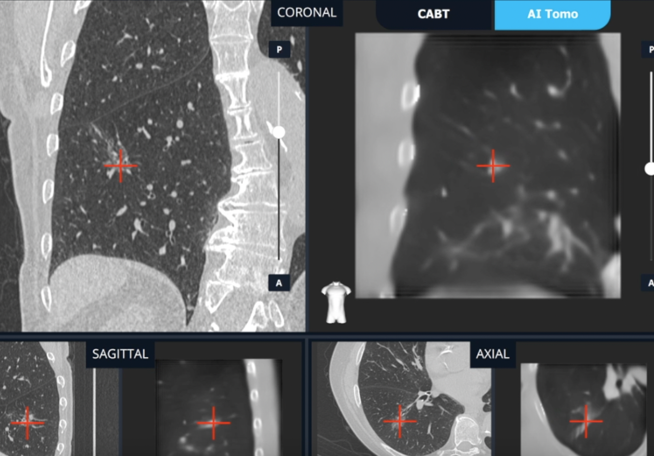
Once the patient is positioned on the table, LungVision registration involves two C-arm spins. The first spin is iso-centered around the main carina, while the second spin is iso-centered around the lesion. These C-arm spins generate an initial C-Arm Based Computed Tomography (CABT) scan, which verifies the precise location of the lesion before proceeding with navigation. In this case, LungVision was paired with a Siemens Cios Spin was used in standard 2D mode, enabling the creation of real-time, intraoperative 3D scans at 17% (1/6th) of the radiation exposure that would have been emitted by a Cios Spin performing a 3D Spin.

Marking the main carina on LungVision’s CABT during registration.

Lesion marking on LungVision’s AI Tomography during registration.
Navigation
The Ethicon MONARCH™ robot’s electromagnetic navigation (EMN) system was used to navigate to the lesion. LungVison’s augmented fluoroscopy provided the missing real-time imaging needed to compensate for CT-to-body divergence and enable precise navigation of the “final mile” to the lesion.
LungVision real-time augmented fluoroscopy and pathway overlay during navigation.
Tool-in-Lesion Confirmation
Once near the target lesion location as defined by the Ethicon MONARCH™ robot, a biopsy needle was introduced down the working channel of the bronchoscope and a third C-arm spin was performed to get visual tool-in-lesion confirmation in multiple 3D planes with LungVision’s intraoperative CT imaging.

LungVision C-Arm Based Tomography (CABT) imaging showing tool-in-lesion confirmation.

LungVision interactive 3D View of the intraoperative CT scan confirming tool-in-lesion confirmation.
Biopsy
LungVision’s augmented fluoroscopy provided real-time imaging during biopsy to confirm tissue samples were acquired from within the lesion.
Needle biopsy performed under LungVision’s real-time, augmented fluoroscopy.
Conclusion
LungVision's intraoperative CT imaging provided the real-time imaging that enabled accurate navigation of the “final mile” to an 18mm GGO, visual confirmation of tool-in-lesion, and image-guided biopsy.
About Dr. Francisco Almeida

Interventional Pulmonology
Cleveland, Ohio