Lesion Characteristics
Lesion Size (diameter): 12mm GGO (5mm Solid /12mm GGO)
Lesion Location: Left Upper Lobe (LUL)
Visible on Fluoro: No
Lesion Density: This semi-solid lesion of -700 Hounsfield units (HU)
Case Information
Full Procedure Time: 3 hours 6 minutes
Anesthesia Start: 10:53
Anesthesia Stop: 13:59
Final Pathology Report
TOTAL SIZE (invasive lepidic components): 1.2 cm
INVASIVE TUMOR SIZE: 0.5 cm
HISTOLOGIC TYPE: Adenocarcinoma, lepidic predominant pattern
Patient Background
77-year-old male with PMH of CHF, HTN, CAD s/p CABG, and stent placement. 40-pack year smoking history. GERD presents for follow-up of repeat CT Chest. The patient's breathing has improved with inhalers. The patient underwent CT of the chest which demonstrated increased progression of LUL ground glass opacities now with some semi-solid lesions.
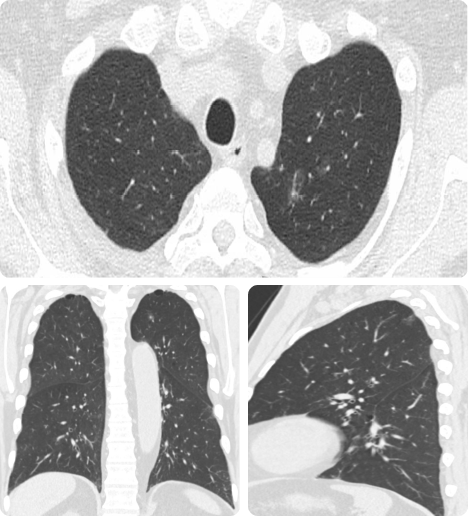
Chest CT showed a 15.2 mm ground-glass opacity (GGO) with two small 1-2 mm nodular solid components in the left upper lobe slightly increased in size and the nodules are new.
Lesion Marking
LungVision’s proprietary artificial intelligence (AI)-driven imaging algorithm intraoperatively generates near-CT quality scans from X-ray images acquired during a C-arm spin. This enabled the visualization and precise dye marking of a semi-solid lesion that had a GGO component of -700 Hounsfield units (HU).

Intraoperative visualization of the GGO under LungVisionTM C-Arm Based Tomography (CABT) imaging.
Dye Marking for Resection
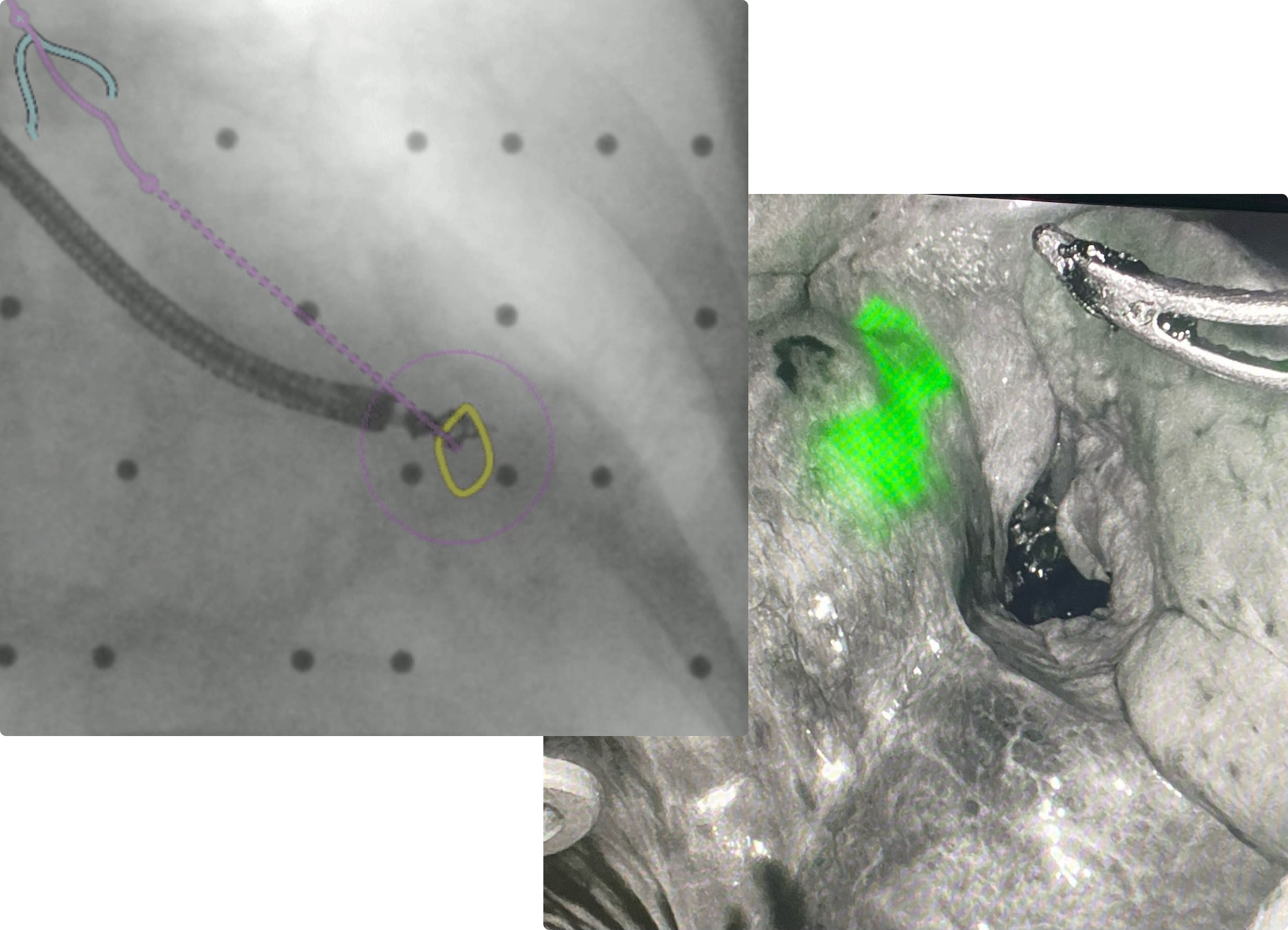
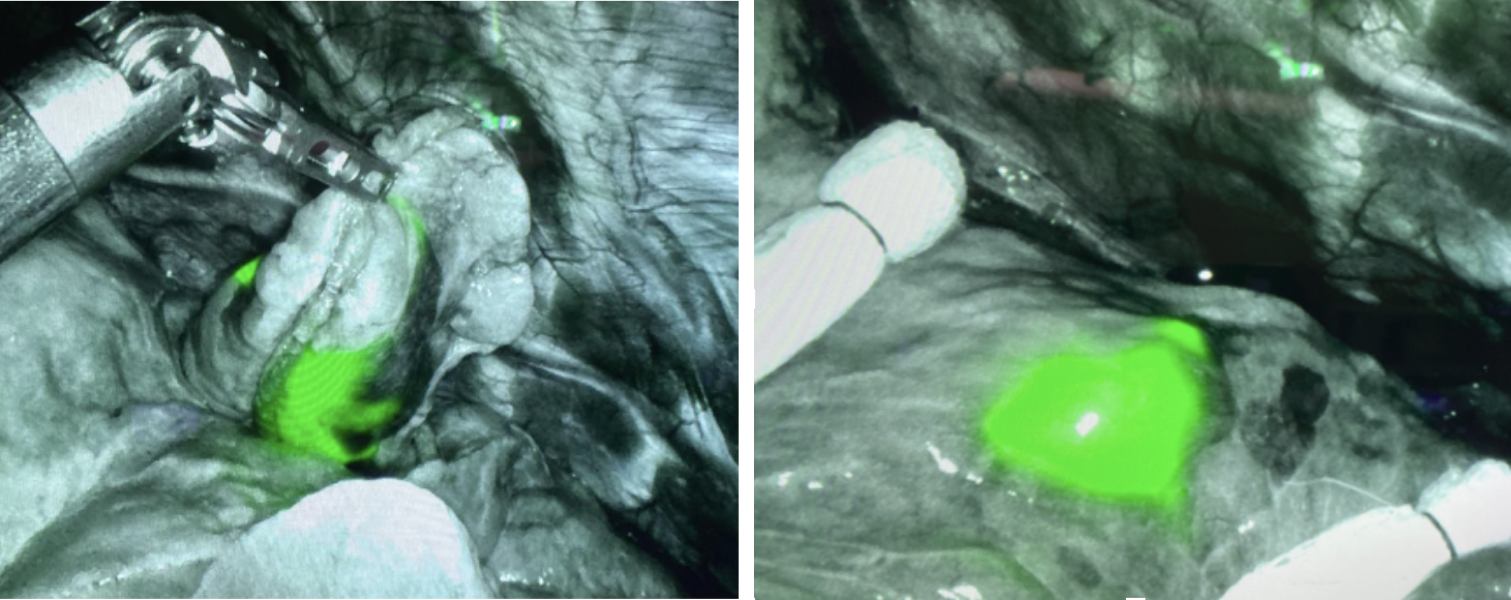
Under LungVision’s real-time augmented fluoroscopy, an indocyanine green (ICG)-soaked coil was placed into the lesion to dye mark the lesion for a subsequent resection.
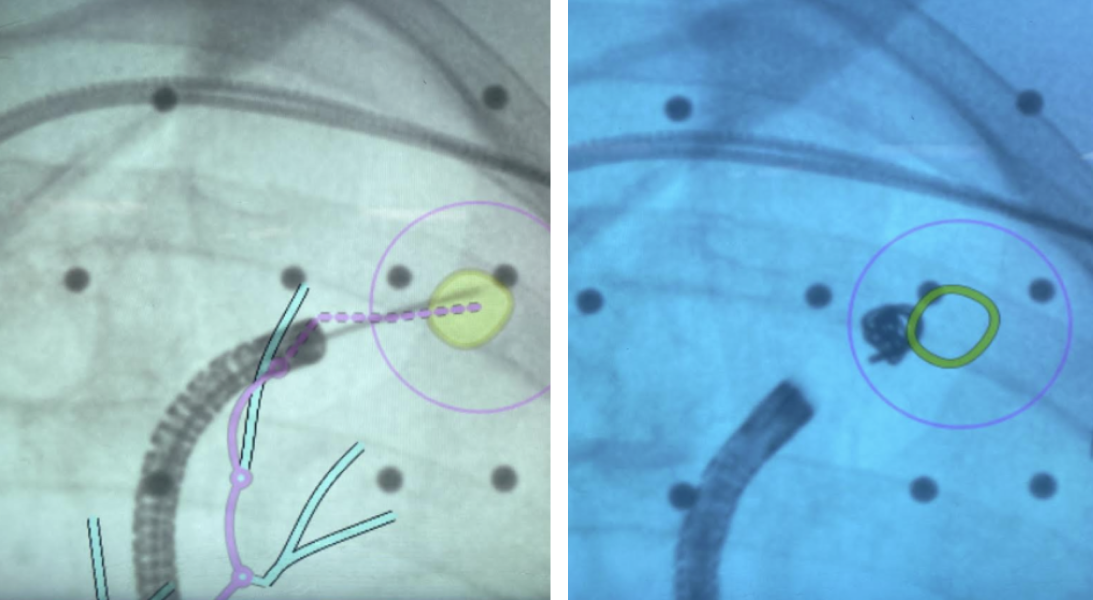 Placement of ICG-soaked coil to dye mark lesion for subsequent resection under LungVisionTM real-time augmented fluoroscopy.
Placement of ICG-soaked coil to dye mark lesion for subsequent resection under LungVisionTM real-time augmented fluoroscopy.
 When the specimen was brought to the pathologist, it was not palpable, and the pathologist deferred to formalin fixation for definitive diagnosis (permanent specimen).
When the specimen was brought to the pathologist, it was not palpable, and the pathologist deferred to formalin fixation for definitive diagnosis (permanent specimen).
Final Pathology
SPECIMEN TYPE AND PROCEDURE: Wedge resection
LATERALITY: Left
TUMOR SITE: Upper lobe
SPECIMEN INTEGRITY: Intact
TUMOR FOCALITY: Unifocal
TUMOR SIZE:
TOTAL SIZE (invasive lepidic components): 1.2 cm
INVASIVE TUMOR SIZE: 0.5 cm
HISTOLOGIC TYPE: Adenocarcinoma, lepidic predominant pattern
HISTOLOGIC GRADE: Not applicable
VISCERAL PLEURAL INVASION: None
TUMOR EXTENSION: Confined to lung
This patient is scheduled for a Robotic Trisegmentectomy/Possible Lobectomy and Mediastinal Lymph Node Dissection in 2 weeks.
Conclusion
LungVisionTM intraoperative CT imaging provided real-time imaging of this semi-solid lesion in order to enable the accurate dye marking needed for resection of the suspicious pulmonary lesion for both diagnosis and treatment in a single-anesthesia event.
About Dr. Tsai

Wilson Tsai, MD
Director, Thoracic Surgical Program
John Muir Health